Surgical Procedures
Surgical procedures are carried out under local anaesthesia in the rooms, conscious sedation or if authorised by your medical aid fund under general anaesthetic.
What should I do before the surgery?
Confirm your date and time of admission
Stop smoking for at least 48 hours before the operation
You are not allowed to drive for at least 24 hours after undergoing general anaesthesia.
Inform us if you suffer from any serious diseases, and or allergies.
Arrange an authorisation number beforehand from your medical aid.
The hospital will supply you with a gown and underwear to wear during the operation.
If a cold or influenza is contracted before the operation date, you should please bring it under our attention.
Avoid taking Aspirin, as this might lead to excessive bleeding and bruising.
If you are younger than 18 years your parent / legal guardian / spouse should accompany you to sign for your operation.
1. You need to be starved for all anaesthetics and sedation for your own safety. No food or liquids may be taken by mouth for at least six (6) hours before the anaesthetic or sedation.
2. This means if you are on the morning list nothing per mouth from midnight. If you are on the afternoon list a light meal before 7am the morning of surgery is allowed (toast or cereal with clear liquid, no fat or meat).
Post-surgery FAQ
While the complete healing process will take a few weeks, the post oral surgery recovery period is relatively quick. It differs with every patient and the different types of surgeries. Dr. Viljoen will provide you with a sick note, according to the severity of the procedure.
Minor Oral Surgery such as a single tooth extraction / biopsy: patient should be functional within 24 -48 hours.
Dental Implants – depending on the procedure, the number of implants placed, whether bone augmentation was required, 3-5 days should be sufficient to recover. However, a 2-week follow-up visit is required to check that healing around the implant is satisfactory.
Impacted wisdom teeth – patients require 5-7 days. It can take up to 3-month for the jawbone to fill up where the tooth was removed.
Facial Trauma and Reconstruction surgery: 6-weeks. 2- and 6-week follow-up visits will be required.
Many patients biggest fear about oral surgery is the pain that can be expected afterwards. How much pain you can expect after surgery can vary depending on how extensive the procedure was that you had done. Dr. Viljoen will prescribe the pain medication necessary to help you recover comfortably. Pain after most oral surgery tends to be mild to moderate and in almost all cases can be managed with over-the-counter medication every 6-8 hours
Mouth and facial swelling will generally be at its peak in the first two to three days. After that, the swelling will gradually go down. Generally, the swelling will be 80% gone in five to seven days. Remember to carefully follow the instructions given to you on the day surgery, to heal as quickly as possible.
Swelling of the gums around the implant is normal after implant surgery, and often the swelling worsens after the first day and peaks about 72 hours after surgery. When multiple implants are placed, swelling, and bruising of the face and neck can sometimes occur. If major swelling occurs that affects vision, the ability to swallow or open one’s mouth wide enough to eat and drink, the patient should contact Dr. Viljoen immediately.
Yes, you can eat. You should always eat something before taking your pain medication and antibiotics to avoid nausea. We recommend that you drink plenty of cold liquids after surgery and follow a soft food diet for at least 2-weeks. Avoid hot foods as it will disturb initial clot formation in the extraction sites. Following the day of the surgery, it’s best to avoid crunchy foods such as popcorn, nuts, and potato chips which break up into little pieces and can get packed down into the extraction sites. If you had dental implants placed, please avoid chewing hard foods with the implant itself for 8 weeks or the healing of the implant will be compromised. The typical implant requires 12-20 weeks of rest from chewing to completely integrate into the jawbone and be ready for a crown.
Your active rinsing with the saltwater recipe provided will begin the day after surgery, and this will help remove any food particles that may be stuck. Rinse after every meal for at least 2-weeks.
On the day of your surgery, do not spit or rinse your mouth. On the day after oral surgery, you can brush your teeth as you would normally again. When brushing, be gentle in the extraction sites as they may be tender for a few days following the procedure. Brush as well as you can and rinse with the saltwater recipe to aid in healing (1/2 teaspoon table salt + ¼ t bicarbonate of soda in 250ml warm water) 3-5 times per day. The use of commercial mouthwash is not recommended during the healing period. Sometimes the doctor will prescribe a mouth rinse to be used twice a day after surgery for one week as well.
In most cases, patients will have a dissolvable suture at the surgical site(s). Sutures typically take 5-15 days to dissolve. In most instances, the stitches are placed at the time of surgery simply to assist with initial control of bleeding and clot formation. This is especially true with wisdom tooth surgery and other tooth extractions. Loss of a stitch is not considered an emergency, even if it came out on the day of surgery. If your surgeon has performed a bone-grafting procedure and the stitches are coming out prematurely, please contact our office so that the doctor may determine whether you need to be seen on that day.
Post-operative nausea and vomiting may occur due to the after-effects of the general anaesthesia and/or the prescribed medications. Treat nausea the same as you would the flu, (e.g. start with sips of clear liquids like water, 7-Up, ginger ale, apple juice). If those stay down, then continue these fluids until the nausea has completely subsided. Also, it is best to stop taking the prescribed medications until the nausea has passed. If after the first few sips the vomiting returns, wait 2 hours, and start the fluids again. If the pain is quite intense, you may take painkillers such as Ibuprofen. If you still feel nauseous after 24 hours, please contact our offices.
It is not unusual to notice small episodes of bleeding for several days after having teeth removed. You can bite on a damp black tea bag (not rooibos) for 10-15 minutes; the tannic acid in tea helps in clot formation. If your mouth is rapidly filling up with blood and the above measures are not helping to slow down the bleeding, call our office for assistance.
Minor bleeding after implant surgery is to be expected. Placement of a gauze pad over the surgical site with mild biting pressure over the site for 30-45 minutes should effectively stop the bleeding. In special cases, such as a patient with high blood pressure or someone who is taking blood thinners, the implant surgical site may bleed for up to 48 hours after surgery. Vigorous bleeding in which the mouth is filling up with blood is not normal after implant surgery, and the patient should contact Dr. Viljoen immediately if this occurs.
Food consumed on the day of surgery should be soft and cool; hot food and liquids may cause increased bleeding and swelling. After the first day, a gradual return to normal diet is acceptable; however, solid food should NOT be chewed directly over the top of the newly placed implant. Small movements of the implant from chewing may disrupt the healing process and cause the implant to fail.
On the day of surgery, vigorous exercise is NOT recommended. Light activity such as walking or indoor house chores is acceptable. After the first day, the patient should be cautious when returning to high impact exercise or outdoor chores as these may increase swelling, bleeding, and pain. Just be aware that if you get your blood pressure up, the surgical site may begin to throb and ache. At which time you want to slow down and take it easy. Pain medication can also have side effects such as dizziness that will negatively affect exercise.
Occasionally the healing cap that was placed over the implant during surgery may become loose during the days or weeks following surgery. If this occurs, there is no cause for alarm.
Contact the office during business hours and arrange to be seen by the surgeon to replace or tighten the healing cap. Please do not wait longer that 24-hours as the gum will start to close over the implant.
Many oral surgeries are covered by general medical aid plans; however, it is subject to available benefits and scheme rules. The best thing to do is get a pre-estimate of the procedure from Dr. Viljoen and then contact your medical aid and see if the procedure, or some of the procedure, costs are covered by your plan
Bone Graft material. When you have a bone graft placed, Dr. Viljoen always overbuilds the graft because he knows you will lose some of the graft. So, you may find pieces of what feels like grit or sand in your mouth for the first week or two of healing.
Most oral surgery procedures can be performed while patients are on blood thinners. Unless Dr. Viljoen has given you specific instructions to do otherwise, please continue to take your medications as prescribed. If you are on Warfarin, we will need a recent INR test prior to surgery.
Surgical Removals (Wisdom and other teeth)
Wisdom teeth or third molars are the last teeth to erupt, usually between the ages of 17 and 25 years. Most people have four wisdom teeth, but it is possible to have fewer or more. It is generally accepted that teeth which remain completely buried or unerupted in a normal position will have to be assessed for their potential to cause harm.
Teeth become impacted due to a lack of space in the dental arch. Their eruption is therefore prevented by gum, bone, another tooth or all three. When teeth are impacted it is best to remove them, as they can cause problems e.g. tooth crowding, infections and pain.
Sometimes the roots of the teeth are lying across the facial nerve that supply your lower jaw with sensation and care should be taken in removing the roots without damaging the nerve.
Should the teeth in the upper jaw lie very high up, the sinus floor could be opened when they are removed. If this happens during the operation, the surgeon will have to close the sinus by creating a flap out of the gums to close the area.
Please adhere to the following instructions as closely as possible, to ensure healing of the sinus: Don’t blow your nose for two weeks; If you must sneeze, then please sneeze through your mouth and nose simultaneously – don’t block your nose to suppress your sneeze! Avoid sniffing very hard. Only use your prescribed nasal spray if your nose feels blocked. If you use it every 4 to 6 hours as advised on the package insert, it will only be effective for 5 days.
Swelling and pain can be expected for about five days and varies from person to person, with the second day usually being the worst. If the swelling, bruising and pain continue for more than five days it is best to book a follow-up appointment.
- An antibiotic, an anti-inflammatory Painkiller and anti-septic mouthwash will be prescribed by the doctor after the operation (please inform the doctor if you are allergic to penicillin). Finish your course of antibiotics and avoid consuming any alcohol while taking medication. Don’t wait until the pain becomes unbearable before taking your pain medication, because then you might need larger dosages to control your pain. Rinse twice daily with the prescribed mouth wash.
- After tooth extraction, it’s important for a blood clot to form to stop the bleeding and begin the healing process. It will help towards a speedy recovery and lead to less bone loss. The blood clot will have a greyish-brown colour after a day or two – this should not be removed, sucked out or fiddled with the tongue, as this will cause a dry socket. That is when the blood clot formed at the extraction site is dislodged and results in irritation and extreme pain.
- Should the wound start bleeding again, take a teabag (black English Tea), wet it under the tap and bite lightly onto it – the pressure of the bite and the tannin in the tea will stop the bleeding by helping the blood to coagulate.
- It is advised to put an ice pack on the side of your face to prevent excessive swelling. This should be done at twenty-minute intervals for the first day after the operation.
- The stitches will dissolve by themselves any time between 5 and 15 days.
- No fluids for at least 1 hour after the operation. Take pain medication immediately with minimal water.
- For 3 hours after the operation no warm fluids or any other food.
- Avoid lying flat on your back, as this might lead to facial swelling. Sleep on 3 pillows for the first 48 hours. This will reduce swelling and bruising.
- Do not smoke for at least 48 hours after the operation as it promotes bleeding and interferes with the healing process.
- Only consume soft foods for the first three days, avoid popcorn or any other food with pips, seeds or peels for a period of 3 weeks.
You should also rinse your mouth with warm salt water (1 teaspoon of salt and ½ teaspoon of bicarbonate of soda dissolved in 250ml of water) as often as your wish or at least after every meal, but do not spit as this promotes bleeding and may dislodge the blood clot, which may result in a dry socket.
Abscesses
A dental/tooth abscess is a localised acute infection at the base of a tooth, which requires immediate attention from your dentist. They are usually associated with acute pain, swelling and sometimes an unpleasant smell or taste in the mouth. More severe infections cause facial swelling as the bacteria spread to the nearby tissues of the face. This is a very serious condition. Once the swelling begins, it can spread rapidly. The pain is often made worse by drinking hot or cold fluids or biting on hard foods and may spread from the tooth to the ear or jaw on the same side.
Damage to the tooth, an untreated cavity, or a gum disease can cause an abscessed tooth. If the cavity isn’t treated, the inside of the tooth can become infected. The bacteria can spread from the tooth to the tissue around and beneath it, creating an abscess. Gum disease causes the gums to pull away from the teeth, leaving pockets. If food builds up in one of these pockets, bacteria can grow, and an abscess may form. An abscess can cause the bone around the tooth to dissolve.
Antibiotics will usually help the pain and swelling associated with acute dental infections. However, they are not very good at reaching into abscesses and killing all the bacteria that are present. The Maxillofacial and oral surgeon will want to remove infected tissue as soon as it is possible, to remove the source of infection and prevent future problems. They might use antibiotics to help them do this, but the physical removal and stopping of potential places for bacteria to hide and grow is very important.
Antibiotics may be prescribed to destroy the bacteria causing the infection. If the infection is not cured, a hole can be drilled into the tooth to drain the infection. If the root of the tooth is infected, a root canal treatment is the recommended procedure (this tries to save your tooth by taking out the infected pulp). An apicectomy will be performed as a last resort to salvage the tooth. If this is unsuccessful the tooth may require extraction.
An apicectomy is a minor procedure to remove the tip (apex) of the root of a tooth. This is only done if a root canal treatment has failed. The procedure may be carried out using either a local anaesthetic, with or without intravenous sedation, or a general anaesthetic in a hospital operating theatre. The choice between the methods will depend upon the degree of difficulty of the procedure, your medical history, and your personal preference.
During the procedure a small “window” is cut (with a scalpel) in the gum over the root of the tooth. Using a dental drill, the area around the end of the root is exposed to determine the amount of root that should be removed. This portion of the root is then removed with the drill. Any infected tissue is removed from around the end of the root of the tooth.
Apicectomies are not very successful and have a 30-40% failure rate that results in the removal of the tooth.
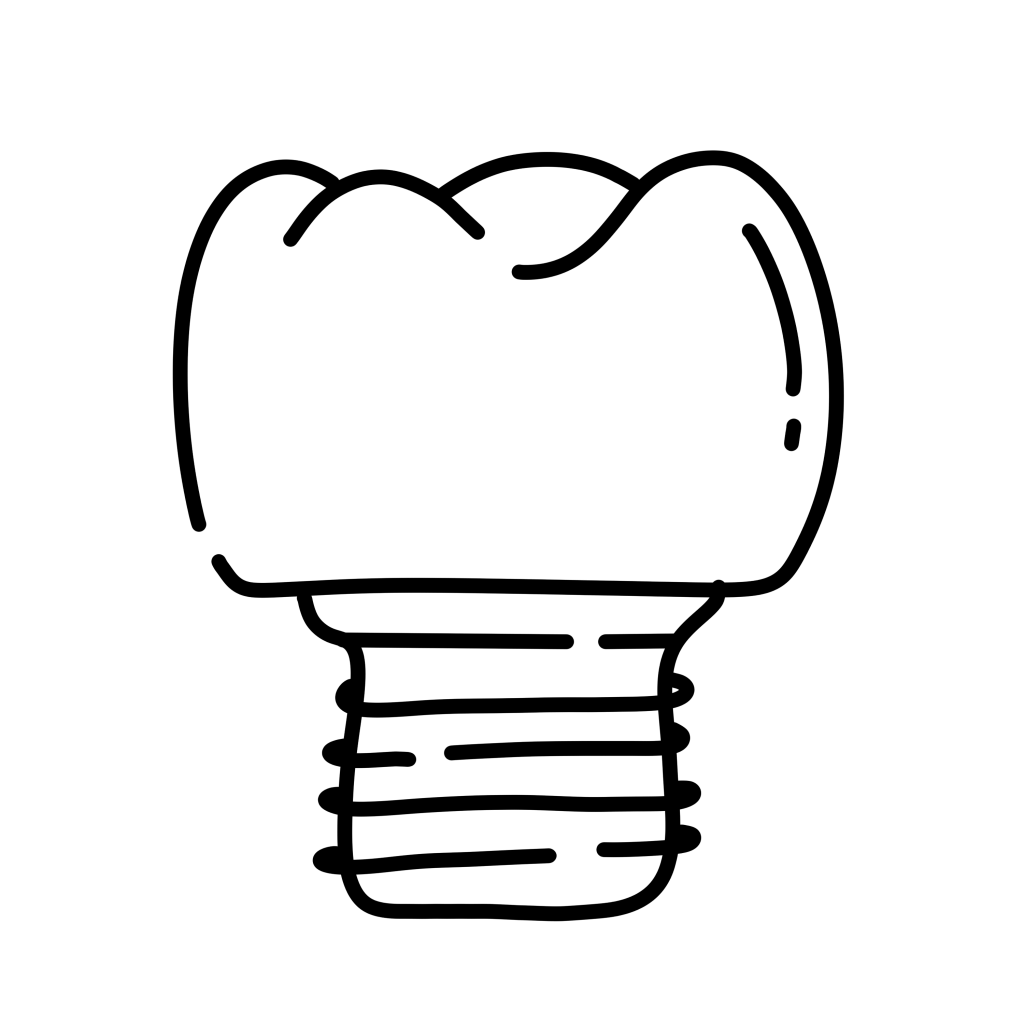
Dental Implants
The decision to proceed with dental implant treatment affects your overall health, appearance, and well-being. We want you to be fully informed about your treatment options and what is involved with the procedures. Please find a summary of the discussion with Dr. Viljoen and the reception staff regarding your treatment plan for the placement of dental implants.
Dental implants are replacement, or substitute tooth roots, used to replace natural tooth roots in areas of the mouth where teeth are missing. It is important to replace the missing tooth as natural tooth roots are embedded in the bone, providing a stable foundation necessary to bite and chew. In essence, the bone holds the tooth roots in place and the roots preserve the bone. When teeth are missing, the bone that previously supported those teeth deteriorates. This process is called bone resorption. However, the bone can be preserved by replacing missing tooth roots with dental implants. Since the bone forms a strong bond to the implants, they can serve the same functions as natural tooth roots.
Dental implants are designed to be permanent; however, many factors contribute to the long-term success of implant treatment, such as home care and regular maintenance visits to the dentist.
The implants are placed in the bone using a gentle surgical technique. Depending upon the stability of the implant, it may or may not be completely under the gum tissue, if a healing abutment is placed. Following the implant placement procedure, the implants are left undisturbed for a period of 5 to 9 months so that the bone can grow around the implants to form a strong biological bond to them. During this bone “integration” phase, you could have some temporary replacement dentures made, so that you never have to be without teeth during treatment.
With implant supported replacement teeth, the appearance of the smile is more natural and the teeth function more like natural teeth. The result is increased comfort and confidence when smiling, speaking, and eating. If dentures and partials are replaced with implant supported teeth, the overall enhancement in quality of life is even more significant, with an ability to eat all types of foods, elimination of messy adhesives, and improved speech, comfort, and appearance. People who wear dentures often worry that their dentures will fall out when they laugh, sneeze and sometimes even when they eat. Since the bone bonds to the implants, replacement teeth have a stable foundation and are securely attached to the implants, so there is no fear that teeth will fall out.
The actual cost of implant treatment is based on several factors: such as the number of teeth being replaced, the type of implant supported teeth recommended and whether additional procedures are necessary to achieve the proper aesthetic and functional result. The overall fees should be calculated based on the complete treatment from consultations with the dentist and maxillofacial and oral surgeon, x-rays, implant placement, cost of implants, other related surgical procedures like bone grafting, fabrication of replacement teeth as well as the estimated components and materials necessary to complete treatment and the dental laboratory fees.
Medical Aid coverage of implant treatment depends on the individual policy. However, it is rare to receive any substantial coverage. Most plans are only designed to cover routine maintenance, emergencies, and basic care with an annual maximum allowable benefit on most plans. Even if an individual policy includes implants as a covered benefit, the amount of coverage is still limited to the annual maximum allowable.
Please note that it is your responsibility as the patient to contact your medical aid to confirm benefits, co-payments and obtain authorisation. If your medical aid declines authorisation for the hospital, please contact us to reschedule an appointment in the rooms.
Dr. Viljoen requires upfront payment of dental implant components prior to the surgery, unless your medical aid can confirm in writing that they will cover the full cost of the components. You will receive an email with a cost estimate for the components the week before your surgery.
- 2-weeks after surgery at no cost. Dr Viljoen will evaluate the healing of the gingiva around the implants and check for any infection.
- 2,5-months after surgery at no cost. Dr. Viljoen will check that the healing abutments are still firmly attached to the implants.
- 5-months after surgery as per attached cost estimate. Dr. Viljoen will remove the healing abutments / surgically remove any gum that cover the implants. He will then insert a special torque wrench to test how strong the implant integrated with the bone.
- You need to obtain a quote and schedule an appointment with your Dentist to take impressions and fit the crown / bridge / denture to the dental implants.
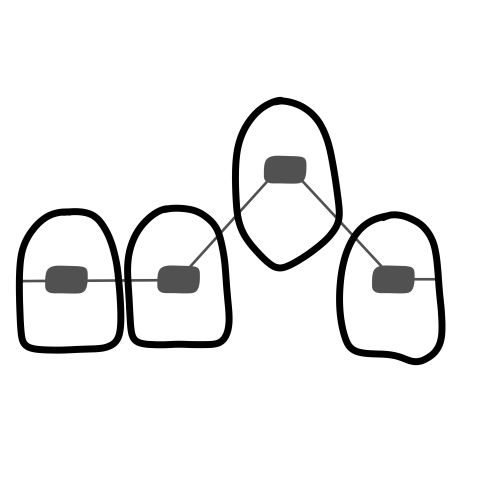
Orthodontic surgery
An impacted tooth simply means that it is “stuck” and cannot erupt into function.
The maxillary canines/eye teeth are the second most common tooth to become impacted. The canine/eye tooth is a critical tooth in the dental arch and plays an important role in your “bite”. The canine teeth are very strong biting teeth and have the longest roots of any human tooth. They are designed to be the first teeth that touch when your jaws close together so they guide the rest of the teeth into the proper bite.
Normally, the maxillary canine teeth are the last of the “front” teeth to erupt into place. They usually come into place around age 13 and cause any space left between the upper front teeth to close tighter together. If a canine/eye tooth gets impacted, every effort is made to get it to erupt into its proper position in the dental arch. 60% of these impacted teeth are located on the palatal (roof of the mouth) side of the dental arch. The remaining impacted eye teeth are found in the middle of the supporting bone, but stuck in an elevated position above the roots of the adjacent teeth or out to the facial side of the dental arch.
In cases where the canine teeth will not erupt spontaneously, the Orthodontist and Maxillofacial and Oral Surgeon work together to get these unerupted eye teeth to erupt. In a surgical procedure performed preferable in hospital, the gum on top of the impacted tooth will be lifted up to expose the hidden tooth underneath. Any bone covering the crown of the tooth will be removed. If there is a baby tooth present, it will be removed at the same time. Once the tooth is exposed, Dr. Viljoen will bond an orthodontic bracket to the exposed tooth. The bracket will have a miniature chain attached to it. He will then guide the chain back to the orthodontic arch wire or adjacent tooth if the arch wire hasn’t been placed yet, where it will be temporarily attached. Sometimes Dr. Viljoen will leave the exposed impacted tooth completely uncovered by suturing the gum up high above the tooth or making a window in the gum covering the tooth. Most of the time, the gum will be returned to its original location and sutured back with only the chain remaining visible as it exits a small hole in the gum.
Shortly after surgery the patient will return to the Orthodontist. A rubber band will be attached to the chain to put a light eruptive pulling force on the impacted tooth. This will begin the process of moving the tooth into its proper place in the dental arch. This is a carefully controlled, slow process that may take up to a full year to complete.
You can expect a limited amount of bleeding from the surgical sites after surgery. Although there will be some discomfort after surgery at the surgical sites, most patients find the prescribed pain medication to be more than adequate to manage any pain they may have. Within two to three days after surgery there is usually little need for any medication at all. There may be some swelling, but it can be minimized by applying ice packs to the lip for the afternoon after surgery. Bruising is minimal after these cases. A soft diet is recommended at first, but you may resume your normal diet as soon as you feel comfortable chewing. It is advised that you avoid sharp food items like crackers and chips as they will irritate the surgical site if they jab the wound during initial healing.
Dr Viljoen recommends that you see your Orthodontist 10-14 days after the surgery to commence pulling on the tooth towards the dental arch.
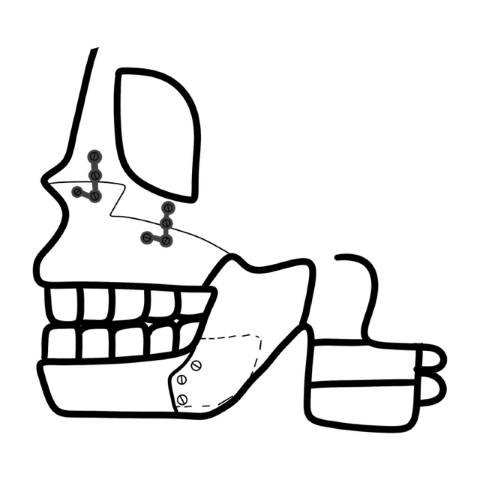
Orthognathic Surgery
Orthognatic surgery, also referred to an Osteotomy, is the cutting into your jawbone to change the structure of it. This occurs when it is not possible to correct your teeth and how they bite together with orthodontics alone. This is because the bones of your face and jaws are out of balance with one another. Surgery (under general anaesthetic) will correct the relationship of the upper jaw to the lower jaw and will rectify these problems. One or more segments of the jaw can be simultaneously repositioned to treat various types of jaw deformities.
The operation is carried out almost entirely from the inside of your mouth so that there are minimal scars on the skin of your face. A cut is made through the gum to gain access to your jawbone. The jaw is then cut with a small saw to allow it to be broken in a controlled manner. It is then moved to its new position and held in place with small metal plates and screws. The gum is stitched back into place with dissolvable stitches that fall out on their own. Occasionally it is necessary to make a small incision on the skin of the face to allow the screws to be inserted. This is very small and usually only requires one stitch to hold it in place.
Immediately after the operation your face will be swollen and will feel tight. Your jaws will be stiff and you will find that you cannot open your mouth widely. The swelling and bruising will improve after about two days, as the second day is usually the worst. You will only be able to have liquids for the first two days after surgery, but soon after that you should be able to progress to a soft diet. In a few weeks after surgery you will be able to eat normal food again. The exact response to surgery is different in each particular case, but in general this is what you can expect.
Oral Pathology / Lesions in the mouth
The inside of the mouth is normally lined with a special type of skin (mucosa) that is smooth and coral pink in colour. Any alteration in this appearance could be a warning sign for a pathological process. The most serious of these is oral cancer. The following can be signs at the beginning of a pathologic process or cancerous growth:
- Reddish patches (erythroplasia) or whitish patches (leukoplakia) in the mouth.
- A sore that fails to heal and bleeds easily.
- A lump or thickening on the skin lining the inside of the mouth.
- Chronic sore throat or hoarseness.
- Difficulty in chewing or swallowing.
These changes can be detected on the lips, cheeks, palate, and gum tissue around the teeth, tongue, face and/or neck. Pain does not always occur with pathology, and curiously, is not often associated with oral cancer.
Lesions are growths or sores that occur in the mouth. These can sometimes resolve themselves after a week or two, and in other circumstances they need to be removed surgically.
- self-induced lesions
- traumatic ulcers
- irritation fibroma
- nicotine stomatitis
- tobacco pouch keratosis
Self-induced lesions are due to habits such as scratching the gum with fingernails or lip, cheek and tongue biting. These usually require a biopsy to confirm the diagnosis.
Traumatic ulcers occur due to a trauma such as biting the lip, cheek, or tongue or from an irritation such as the sharp edge of dentures. Such lesions normally heal by themselves within 7-14 days however if they don’t, a biopsy is indicated.
Irritation fibroma is a lesion composed of dense, scar like connective tissue as a result of chronic trauma or habitual cheek biting or chewing. It is surgically removed and sent for a biopsy to confirm the diagnosis.
Nicotine stomatitis is a lesion induced by heavy smoking. Keratinization occurs resulting in raised red dots on the salivary glands. Tobacco pouch keratosis results in a white lesion from chewing tobacco. This lesion often disappears when tobacco is no longer chewed. In both nicotine stomatitis and tobacco pouch keratosis the smoking can cause an increased risk of squamous cell carcinoma (cancer), as well as an increased risk of caries, periodontal disease, attrition and staining of the teeth.
Oral cancer occurs in the mouth, where the disease can affect the lips, tongue, cheeks and throat. It most commonly involves the tissue of the lips or the tongue, but can also occur on the floor of the mouth, cheek lining, gingiva (gums) or palate (roof of the mouth). Most oral cancers look very similar under the microscope and are called squamous cell carcinomas. These are malignant and tend to spread rapidly.
Anyone can be affected by oral cancer, but it is most common in men over the age of forty.
Most cases of mouth cancer are linked to tobacco and alcohol. Chewing tobacco is very dangerous and if tobacco and alcohol are consumed together the risk is even greater.
Excessive exposure to sunlight increased the chance of developing lip cancer.
The human papilloma virus (HPV) plays a big role in the development of oral cancers.
• Any sores on the face, neck or mouth that do not heal in a month.
• Swelling, lumps or bumps on the lips, gums or other areas inside the mouth.
• White, red or dark patches in the mouth.
• Repeated bleeding in the mouth.
• Numbness, loss of feeling or pain in any area of the face, neck or mouth.
• Teeth that become loose or even fall out spontaneously might also be a warning sign.
Your dentist should normally do a mouth examination when he sees you every 6 months and any sign of cancer should be picked up.
If you suspect you have cancer, or your dentist thinks that you may have it, you can come in and have a biopsy that is sent off to the pathology lab and it takes 2-3 working days to get the results. After we receive the results we will phone you and let you know the outcome, and advise you on what steps to take from there.
When the cancer is detected early the success rate for curing it is nearly 75%, unfortunately more than 50% of oral cancers are advanced by the time the cancer is detected. Surgical excision of the tumor is usually recommended if the tumor is small enough. Radiation therapy and chemotherapy would likely be used when the tumor is larger and has spread to the lymph nodes in the neck.
Temporomandibular Joint Disorder (TMJ)
The temporomandibular joint (TMJ) connects the lower jaw called the mandible, to the temporal bone at the side of the head. There are two TMJs, one on each side of the jaw and are flexible so that the jaw can move smoothly, allowing us to talk, chew and yawn. Muscles attached to and surrounding the jaw joint controls its position and movement. When we open our mouth, the rounded ends of the lower jaw joint, called condyles, glide along the joint socket of the temporal bone. These condyles slide back into place when we close our mouth. To keep this motion smooth a soft, shock-absorbing disc made of cartilage lies between the condyle and temporal bone. These parts make up the TMJ.
TMJ disorders are a group of medical problems related to the jaw joint. There are three main categories of TMJ disorders; they are muscle disorders, derangement disorders and degenerative disorders. The muscle disorders, include pain in the muscles that control jaw function, as well as pain in the muscles of the neck and shoulders. Derangement disorders relate to derangement of the TM joint, such as a dislocated jaw, displaced disk or injured bone. The last, degenerative disorders include wear and tear of the TM joint, often caused by arthritis and this leads to destruction of the cartilage that covers the TM joint.
TMJ disorders may be caused by injuries, deterioration due to aging, and behavioural factors. Symptoms of the disorder include headaches, ear pain, bite problems, clicking sounds and locked jaws. A heavy blow to the jaw could fracture the bones of the joint or damage the disc, disrupting the smooth motion of the jaw and cause pain or locking of the joint. Aging problems, such as arthritis, regular gum chewing can cause wear and tear of the joint. Teeth grinding and clenching can increase wear on the cartilage of the TM joint, which can lead to ear and jaw pain. Abnormal position or missing teeth (malocclusion) plays an significant role in the deterioration of the joints and often orthodontic treatment or replacement of molar teeth with dental implants of partial dentures are needed to improve the symptoms.
Conservative treatment such as rest, heat and ice treatment, physical therapy and anti-inflammatory medications are the best place to start. In order to rest your jaw, avoid hard or chewy foods or opening your mouth too wide. A splint or bite plate can be used to reduce clenching and grinding, which will ease muscle tension. If none of these treatments seem to help, occlusal appliances can be used to relax muscles, stabilize and protect the joint and relieve the load on the disk. In extreme cases surgical replacement of jaw joints with artificial implants can be done, but this is still a controversial treatment
Salivary Gland Diseases
Your salivary glands produce as much as a 1.5 litre of saliva each day. Saliva is important to lubricate your mouth, help with swallowing, protect your teeth against bacteria, and aid in the digestion of food. The three major pairs of salivary glands are:
- Parotid glands on the insides of the cheeks
- Submandibular glands at the floor of the mouth
- Sublingual glands under the tongue
There are also several hundred minor salivary glands throughout the mouth and throat. Saliva drains into the mouth through small tubes called ducts.
When there is a problem with the salivary glands or ducts, you may have symptoms such as salivary gland swelling, dry mouth, pain, fever, and foul-tasting drainage into the mouth. Salivary stones can interfere with the function of the salivary glands or block the ducts so they can’t drain saliva. When saliva can’t exit through the ducts, it backs up into the gland, causing pain and swelling that gets progressively worse. Unless the blockage is cleared, the gland is likely to become infected.
Bacterial infection of the salivary gland, most commonly the parotid gland creates a painful lump in the gland, and foul-tasting pus drains into the mouth. It is more common in older adults with salivary stones, but it can also happen in babies during the first few weeks after birth. If not treated, salivary gland infections can cause severe pain, high fevers, and abscess (pus collection). Bacterial infections generally cause one-sided salivary gland swelling. Cysts can develop in the salivary glands if injuries, infections, tumours, or salivary stones block the flow of saliva
Viral infections such as mumps, flu, and others can cause swelling of the salivary glands. Swelling happens in parotid glands on both sides of the face, giving the appearance of “chipmunk cheeks.” It usually begins approximately 48 hours after the start of other symptoms such as fever and headache. Other viral illnesses that cause salivary gland swelling could include for example the Epstein-Barr virus, cytomegalovirus, Coxsackievirus, and the human immunodeficiency virus.
Several different types of tumours can affect the salivary glands. They can be cancerous (malignant) or noncancerous (benign). The two most common tumours are pleomorphic adenomas and Warthin’s tumour. Pleomorphic adenomas most commonly affect the parotid glands, but can also affect the submandibular gland and minor salivary glands. The tumour is usually painless and grows slowly, are benign (noncancerous) and are more common in women than men. Warthin’s tumour is also benign and affects the parotid gland. Warthin’s tumour can grow on both sides of the face and affects more men than women.
Sjögren’s syndrome is a chronic autoimmune disease in which cells of a person’s immune system attack the salivary and other moisture-producing glands, leading to dry mouth and eyes. About half of people with Sjögren’s syndrome also have enlargement of the salivary glands on both sides of the mouth, which is usually painless.
Treatment for salivary gland problems depends on the cause. For stones and other blockages of the ducts, treatment begins with the manual removal of stones, warm compresses, or sour candies to increase the flow of saliva. If simple measures don’t relieve the problem, surgery may be required. Surgery is usually required to remove large cysts and benign/malignant tumours. Some benign tumours are treated with radiation to keep them from coming back. Some cancerous tumours require radiation and chemotherapy. Other problems may be treated with medications only. For example, bacterial infections are treated with antibiotics. Medications can also be prescribed for dry mouth.
Trauma & Facial Injuries
Maxillofacial injuries also referred to as facial trauma, encompass any injury to the mouth, face and jaw. There are a number of possible causes of facial trauma such as motor vehicle accidents, accidental falls, sports injuries, interpersonal violence, and work-related injuries. Typically, facial injuries are classified as either soft tissue injuries (skin and gums), bone injuries (fractures), or injuries to specific regions (such as the eyes, facial nerves or the salivary glands).
Injuries can vary from a dislodged (bumped out) tooth/teeth to complex combination of fractures of the bones of the face i.e. the lower jaw, upper jaw, palate, cheekbones, eye sockets and combinations of these bones.
These injuries can affect sight, the ability to breathe, speak and swallow. Treatment often requires hospitalisation and cannot be fixed immediately, as the swelling needs to subdue, and more serious injuries need to be treated first.
The fracture is treated under general anesthetic by placing plates and screws in place to hold the fractured bone segments together. This is done in a manner to ensure that the fewest number of scars are left on the face. This technique is called “rigid fixation” of a fracture. The relatively recent development and use of rigid fixation has profoundly improved the recovery period for many patients, allowing them to return to normal function more quickly. An attempt at accessing the facial bones through the fewest incisions necessary is always made. At the same time, the incisions that become necessary, are designed to be small and, whenever possible, are placed so that the resultant scar is hidden.
Once it is completely healed (this takes about two months) the plates and screws may be removed. Additional operations may be required after 6-12 months to ensure a pre-treatment facial structure.
When soft tissue injuries such as lacerations occur on the face, they are repaired by suturing. In addition to the obvious concern of providing a repair that yields the best cosmetic result possible, care is taken to inspect for and treat injuries to structures such as facial nerves, salivary glands, and salivary ducts (or outflow channels).
Maxillofacial and Oral Surgeons are trained, skilled and uniquely qualified to manage and treat facial trauma. Injuries to the face, by their very nature, impart a high degree of emotional, as well as physical trauma to patients. The science and art of treating these injuries requires special training, involving a “hands on” experience and an understanding of how the treatment provided will influence the patient’s long term function and appearance.
After the fractures have been repaired, a healing time of between 4-6 weeks (often longer in more extensive cases) should be allowed. During this time the patient will need to follow a diet that is adapted to his/her own special circumstances and can differ from a strict fluid diet to a diet of semi-solid foods. Special attention to oral hygiene is essential. Physiotherapy is also valuable in the rehabilitation, especially in injuries of the jaw-joint or extensive skin and muscle injuries.